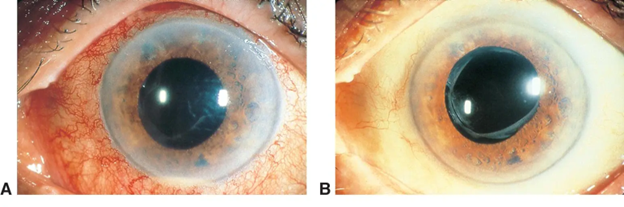
A 34-year-old woman presents with photophobia and dull eye pain
Cataract/Anterior Segment
What is your diagnosis?
The diagnosis is...
![]()

The image and history are consistent with a diagnosis of iritis.
- It is most commonly idiopathic, but it may occur with autoimmune conditions including those associated with the HLA-B27 genotype, sarcoidosis, juvenile idiopathic arthritis (JIA), and Behçet disease. Infectious etiologies including syphilis, herpes simplex virus (HSV), and varicella-zoster virus (VZV) should also be considered.
- It can present with dull, progressive eye pain, conjunctival hyperemia, tearing, and photophobia.
- Potential complications include cataracts, macular edema, and secondary glaucoma.
What is the role of the primary care or emergency medicine physician?
![]()
- Obtain a complete history to evaluate for infectious versus autoimmune etiologies of iritis.
- Rule out vision-threatening causes of a red, painful eye such as trauma.
- Refer for evaluation by an ophthalmologist for a complete eye examination and thorough workup.
What is the role of the ophthalmologist?
![]()
- Perform a slit-lamp evaluation, which may demonstrate these characteristics:
- Cell and flare in the anterior chamber
- Keratic precipitates on the corneal endothelium
- Corneal clouding
- Altered pupil shape and reaction to light
- Rule out vision-threatening conditions such as acute angle-closure glaucoma.
- Test for infectious and autoimmune etiologies.
What is the treatment?
![]()
Treatment selection depends on symptom severity and cause:
- Topical cycloplegic medications are used to dilate the pupil, reducing pain and preventing synechiae to the lens.
- Topical steroids may be used to reduce inflammation.
- Topical intraocular pressure-lowering drops can be used if necessary.
- If the cause is infectious or autoimmune, treatment of the underlying etiology is required.
Learn more: Ophthalmology resources for medical students
![]()